
Introduction
| Div | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||
|

| Div | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||
|

| Div | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||
|

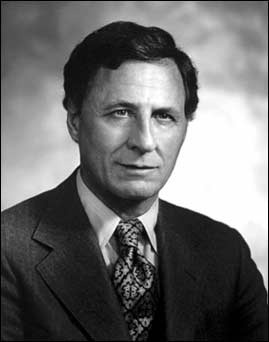
Edward Driscoll of NIDR's1 Oral Medicine and Surgery Section began conducting studies of dental anesthesia in 1957. His aims were: to establish the necessary baseline physiological data; to evaluate the effects of stress on the dental patient; and to find the best methods of alleviation. With his associates, he performed full mouth extractions on more than 1200 patients, and collected readings for pulse, blood pressure, respiration, arterial oxygen levels, EEG, and EKG. Edward Driscoll. Photograph courtesy of NIDCR Public Information Office.
...
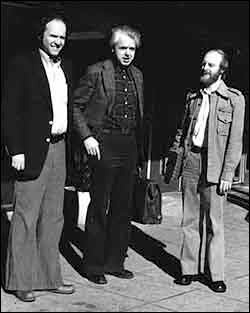
Ron Dubner and the "Lone Rangers"
| Div | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||
|

...
Overview
Content Tools
ThemeBuilder